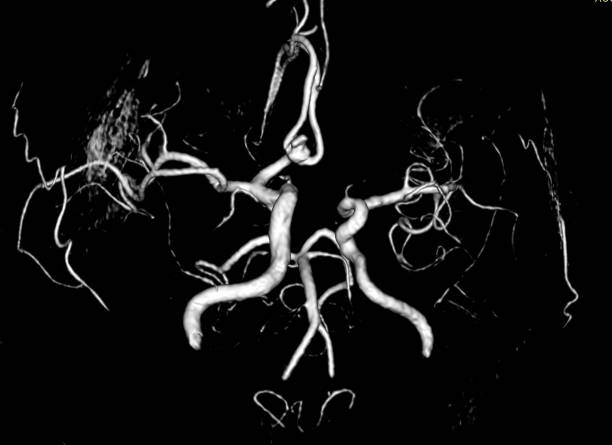
Getting an angiography result that confirms a blockage is the moment most patients dread. The mind races straight to surgery, to long recovery periods, and to worst-case outcomes. What most people do not realise is that a positive blockage report does not automatically mean an operation. The decision ahead is layered, deliberate, and highly individual to the patients overall health conditions.
Treatment after angiography depends on how many arteries are blocked, the degree of narrowing, and whether the heart muscle is under active threat. Patients who seek care at a heart specialist hospital in Ranchi benefit from coordinated expertise across cardiology, interventional procedures, and cardiac surgery, all working from the same diagnostic findings to determine which path carries the least risk and the best long-term outcome.
When Medication Is the Appropriate First Step
Stable Disease With Manageable Risk: Not every blockage demands a procedure. When narrowing falls below a critical threshold and the patient is not experiencing significant symptoms or evidence of reduced blood supply to the heart, doctors typically begin with medical management. Statins, anti-platelets, beta-blockers, and targeted lifestyle changes can stabilise plaque and reduce cardiac risk over time without the need for intervention.
Monitoring Progress Without Rushing to Intervene: Medical therapy is not a passive choice. Doctors track patients on medication through periodic stress tests and imaging to assess whether the blockage is progressing or holding stable. If symptoms worsen or functional testing reveals increasing blood flow compromise, the treatment plan is revisited. Medicine often buys critical time and sometimes removes the need for any further procedure at all.
See also: How Commercial Pest Control Works (And Why It Is Different
The Anatomy of an Angioplasty Decision
Single-Vessel Blockage and the Role of Flow Assessment: When a single artery shows significant narrowing and the patient has symptoms such as chest pain on exertion or a positive stress test, angioplasty with stenting is often the preferred route. Cardiologists may measure fractional flow reserve to confirm whether the blockage is genuinely restricting blood flow before placing a stent, which avoids unnecessary procedures in borderline cases.
Emergency Situations That Remove the Decision Window: In an acute heart attack caused by a sudden complete closure of an artery, there is no debate about treatment. Immediate angioplasty is life-saving. Every minute without restored blood flow increases permanent muscle damage, so catheterisation laboratories in high-volume cardiac centres must function around the clock. Speed and a skilled interventional team determine the outcome more than any other factor.
What Angioplasty Cannot Always Solve: Angioplasty works well for discrete, accessible blockages but has clear limitations. Heavily calcified lesions, very long segments of disease, or blockages near complex branching points may not respond reliably to stenting alone. In these cases, proceeding with angioplasty can create more problems than it resolves, and the input of a cardiac surgeon becomes a necessary part of the conversation.
Bypass Surgery: When the Stakes Are Too High for Stenting Alone
Multi-Vessel Disease and the Long-Term Picture: When angiography reveals blockages in two or three major coronary arteries, or when the left main coronary artery is critically narrowed, bypass surgery often produces better outcomes over a decade compared with stenting. This is especially true in patients with diabetes, where stents carry a higher rate of re-narrowing. Surgeons create new pathways using vessels from the chest or leg.
Reduced Heart Function and Surgical Planning: Patients with significantly reduced left ventricular ejection fraction, meaning the heart is pumping well below its normal capacity, often require surgery rather than angioplasty. Bypass can restore blood flow to a larger territory of heart muscle, which may improve pump function over time. This nuanced calculation involves imaging specialists, interventional cardiologists, and surgeons reviewing findings together before any final plan is confirmed.
Key Indicators Doctors Weigh Before Making a Recommendation:
- Number Of Arteries Affected: Triple-vessel disease almost always favours surgical revascularisation over repeated stenting.
- Degree Of Blockage: Narrowing beyond 70% in a major vessel typically signals a need for active intervention rather than medication alone.
- Heart Muscle Viability: When imaging confirms oxygen-starved tissue, restoring blood flow through surgery may recover function.
- Patient Comorbidities: Conditions such as chronic kidney disease or advanced age shift the risk calculation toward less invasive options.
- Symptoms At Rest: Chest pain or breathlessness without physical exertion is a clear signal that medication alone is unlikely to suffice.
The Conversation No Patient Should Have Alone
Getting a Second Opinion Is Not a Sign of Doubt: When the path forward is unclear, or when a patient has been advised surgery but remains uncertain, seeking input from another specialist is entirely appropriate. Cardiac care decisions are complex enough that even experienced cardiologists rely on formal Heart Team discussions before recommending bypass surgery. A second perspective does not delay care. It often makes the final recommendation far more confident.
Questions Worth Raising Before Any Procedure: Patients are not expected to absorb everything at once. Asking questions before committing to a treatment plan is not merely a right, it is a necessity. Which arteries are blocked and by how much? What are the realistic outcomes of medication alone? These are not disruptive questions. They tend to lead to calmer, better-informed decisions.
A Blockage Report Is the Beginning, Not the Last Word
Understanding what an angiography result means is the first step toward a calmer, more informed conversation with a care team. Treatment choices reflect clinical evidence, individual risk profiles, and the collective expertise of specialists who assess the full picture together. If you or someone in your family has received a blockage report, consult a qualified cardiologist without delay to explore your options with complete clarity.